
Advocating for Yourself at the Doctor's Office
Why This Is Harder Than It Should Be
You have been experiencing something real. Disrupted sleep, mood shifts, brain fog, irregular cycles, symptoms you know are not normal for you. You made the appointment. You sat in the waiting room. And then you left feeling like you weren't heard, or worse, like you were told everything was fine when it clearly wasn't.
This is not an uncommon experience.
A survey by the North American Menopause Society found that 45% of women reported that their healthcare provider did not take their menopause symptoms seriously. A separate 2025 national survey of over 1,000 U.S. women found that nearly 40% reported being misdiagnosed when they sought care for perimenopause symptoms.
Women described feeling "dismissed," "brushed off," and told they were "too young" to be experiencing what they were experiencing. Some were told to simply accept it.
Understanding why this happens does not excuse it, but it does help you prepare for it.
The Training Gap Is Real
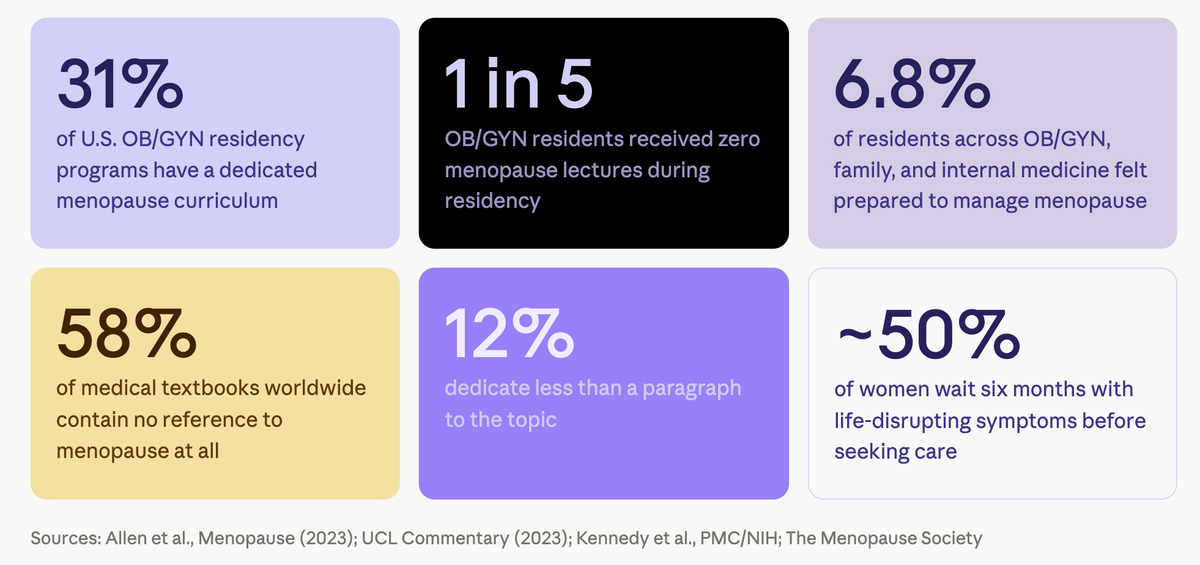
Part of the problem is structural. Only 31.3% of U.S. OB/GYN residency programs have a dedicated menopause curriculum. One in five OB/GYN residents reported receiving no menopause lectures during residency at all. Among family medicine, internal medicine, and OB/GYN residents, only 6.8% felt adequately prepared to manage women experiencing menopause.
One study found that 58% of medical textbooks used around the world had no reference to menopause, and 12% dedicated less than a paragraph to the topic.
This is not an excuse for poor care. But it does mean that your healthcare provider may genuinely not know what you are experiencing, and it means that how you show up to appointments matters more than it should.
About half of women wait six months with life-disrupting symptoms before seeking care.
You deserve better than that. Here is how to close the gap.
Before Your Appointment
Track your symptoms in writing
A verbal description of "feeling off" is easy to dismiss. A written log of specific symptoms, their frequency, their severity, and their impact on your daily life is much harder to set aside.
Before your appointment, aim to track for at least six to eight weeks, ideally covering more than one full cycle. Perimenopause symptoms fluctuate week to week and month to month, so a shorter window can be misleading. If you have been experiencing symptoms for several months already, bring as much of that history as you can. The longer the record, the clearer the pattern.
- Which symptoms you are experiencing and how often
- How severe they are
- What time of day or month they tend to be worse
- How they are affecting your sleep, work, mood, and relationships
- How long this has been going on
If you use My Village to track your symptoms, bring that data with you. Patterns over time are more meaningful than a single snapshot, and they give your provider something concrete to engage with.
This matters more in perimenopause than at almost any other stage of life. Because symptoms fluctuate hormonally (better some weeks, worse others) a single appointment snapshot can be genuinely misleading. A provider who sees you on a good day may not see what you're living with the rest of the time. Consistent tracking over weeks and months closes that gap. It also makes you harder to dismiss. "I've been tracking this for three months and here is what I found" is a different kind of statement than "I've been feeling off lately."
Know your cycle history
Bring information about how your cycle has changed. Irregular cycles are one of the clearest signs of perimenopause. Note any changes in length, flow, frequency, or consistency over the past year or two.
The more data you bring, the less the appointment depends on how well you describe something in the moment, under time pressure, in a clinical setting, possibly while not feeling your best. Your records do the heavy lifting. Think of it as building a case file for your own health. A few weeks of notes is anecdotal. Months of tracked data, showing exactly when symptoms spike, how they connect to your cycle, how they are trending, is something a healthcare provider has to engage with.
Write down your questions in advance
In the moment, it is easy to forget what you meant to ask. Write your questions down before you go, in order of priority, so that even if you only get through half of them, you've covered what matters most.
Know your family history
Your mother's experience with perimenopause and menopause is relevant clinical information. If she had an early transition, significant symptoms, or cardiovascular or bone health concerns after menopause, that is worth raising.
At the Appointment

Lead with your most impactful symptoms first
Appointments are short. Do not build to your main concern. Open with the symptom that is most affecting your quality of life, and say so explicitly: "The main reason I'm here is that I haven't slept properly in three months and it's affecting my ability to function at work."
Framing your symptoms in terms of functional impact (what you can no longer do or do well) tends to land differently than listing symptoms in isolation.
Be specific about timeline and severity
"I've been feeling anxious" is less actionable than "I've been waking up at 3am with a racing heart two or three nights a week for the past four months, and I've never experienced anxiety like this before." Specificity signals that you have been paying attention and that this is not a vague or passing concern.
Say it out loud if you think it's perimenopause
Research found that some women were told they couldn't be experiencing perimenopause-related symptoms because of their age or because their cycles were still regular. Neither of these things rules out perimenopause. Symptoms can begin years before cycles become irregular, and perimenopause can start in the late 30s.
If you suspect perimenopause, say so directly: "I've been researching perimenopause and I think that may be what I'm experiencing. I'd like to talk through that possibility."
You are not diagnosing yourself. You are opening a door that your provider may not have thought to open.
Ask for what you need
Do not wait to be offered next steps. Ask:
- "What do you think might be causing these symptoms?"
- "Could this be perimenopause?"
- "What would you recommend as a next step?"
- "Are there tests we should run to rule other things out?"
- "Is there a specialist you would recommend I see?"
- "What are my options, including non-hormonal and hormonal approaches?"
If your provider mentions hormone therapy or declines to mention it, it is reasonable to ask about it directly. There are multiple treatment approaches for perimenopause symptoms, and you are entitled to understand all of them.
If you feel dismissed, name it
This is uncomfortable, but it works. If you feel like your concern is being minimized, it is appropriate to say calmly: "I want to make sure I'm communicating how much this is affecting my daily life. I'm not looking for reassurance. I'm looking for a path forward."
You can also ask: "Is there something more I should be sharing to help you understand what I'm experiencing?"
After the Appointment
Follow up in writing
If your provider gave you information, a referral, or a treatment recommendation, send a brief follow-up message summarizing what you understood. This creates a record and catches any miscommunication early.
Seek a second opinion if you need one
If you left the appointment feeling dismissed, unheard, or worse than when you went in, a second opinion is not a betrayal. It is appropriate healthcare.
Some women find it helpful to specifically seek out a Menopause Society Certified Practitioner (MSCP), a healthcare provider who has completed specialized training in menopause care. This does not guarantee a perfect experience, but it does mean you are seeing someone with dedicated knowledge in this area. You can search for certified practitioners at menopausesociety.org.
Track what changes (or doesn't)
If you are given a recommendation, keep tracking your symptoms so you can report back with specifics. "I tried that and it didn't help" is less useful than "I tried that for six weeks and my sleep improved but the mood symptoms are the same." Specific feedback leads to better follow-up care.
The Bigger Picture
Change is happening. The Menopause Society is actively pushing for standardized menopause curriculum in residency programs. Certified practitioners are a growing presence. The science on perimenopause has expanded significantly in recent years.
But the system has not yet caught up for most women navigating their 40s in a standard primary care setting. Until it does, preparation is your best tool.
Tracking your symptoms, writing down your questions, leading with your most impactful concerns, and being willing to name it when you're not being heard are not workarounds. They are the difference between an appointment that moves things forward and one that doesn't.
My Village is built to help you build that case. The more clearly you understand your own patterns over time, the better equipped you are to make sure the people caring for you understand them too. That record is yours. It travels with you to every appointment, every second opinion, every new provider. Start building it now.
References used in this post:
- North American Menopause Society — 45% of women not taken seriously by providers: cited in ksat.com
- Biote 2025 National Survey — 40% misdiagnosed: oova.life
- Allen, J.T. et al. — Needs assessment of menopause education in U.S. OB/GYN residency programs, Menopause (2023): pubmed.ncbi.nlm.nih.gov
- The Menopause Society / Faubion, S. — Residency training gaps: contemporaryobgyn.net
- UCL Commentary — Medical school menopause education gaps (2023): ucl.ac.uk
- Kennedy et al. / Women Living Better Survey — Seeking healthcare for perimenopausal symptoms, PMC/NIH: pmc.ncbi.nlm.nih.gov
- General practitioners' and women's experiences of perimenopause consultations, PMC/NIH: pmc.ncbi.nlm.nih.gov
My Village is a wellness platform, not a medical service. Nothing here is medical advice. If you are experiencing symptoms that concern you, please speak with a qualified healthcare provider.
Related Articles
Perimenopause and Menopause at Work: Why Normalizing This Conversation Is Good for Everyone
Perimenopause and menopause are costing organizations their most experienced talent. Learn why workplaces need to normalize this conversation, what employers and HR leaders can do right now, and where to find free resources across North America and globally.
Nobody Said the Word Hormones
A My Village co-founder spent years being told her test results were inconclusive. Broken sleep, weight gain, heart palpitations, and brain fog, yet nobody mentioned perimenopause. Her story of falling through the gaps of women's health, and what changed when someone finally listened.
Brain Fog in Perimenopause: What's Happening and What to Do
Forgetting words, losing your train of thought, struggling to focus? Brain fog during perimenopause is real, and it has a biological basis. Here's what the research says and what actually helps.